|
"Cheap 40mg lasix with amex, blood pressure normal variation". By: L. Will, M.B. B.CH. B.A.O., Ph.D. Co-Director, Alpert Medical School at Brown University
Buy lasix 40 mg low costThe only other central gray-m at ter structure is the thalam us blood pressure medication usa best order lasix, which is prim arily sensory ("gateway to consciousness") and is involved solely secondarily pre hypertension and diabetes buy lasix with a mastercard, through suggestions m echanism s blood pressure medication causing dizziness order 100mg lasix amex, in m otor sequences arteria coronaria dextra purchase generic lasix canada. The three largest m otor nuclei are as follows: � Caudate nucleus � Putam en � Globus pallidus (developm entally, part of the diencephalon) these three nuclei are som etim es recognized by various collective designations: � the lentiform nucleus is form ed by the putam en, globus pallidus, and intervening ber tract s. In addition to these three nuclei, there are other nuclei which may be thought of functional part s of the m otor system (also proven here). In a strictly anatom ical sense, only the telencephalic constructions listed above are constituent s of the basal nuclei (ganglia). Som e textbooks m istakenly embody the subthalamic nucleus of the diencephalon (see p. Functional disturbances of the basal nuclei are characterized by m ovem ent disorders. Functiona l Systems Supplem entary m otor cortex Prim ary m otor cortex Som atosensory cortex Prem otor cortex Parietal lobe Cortical efferent fibers to brainstem and spinal cord Thalamus Centrom edian nucleus Ventral lateral nucleus Subthalam ic nucleus Putam en Globus pallidus, lateral segm ent Globus pallidus, m edial segm ent Compact half Reticular half Substantia nigra B Flow of information betw een motor cortical areas and basal gang lia: motor loop the basal ganglia are involved with the controlled, purposeful execution of ne voluntary movements. They combine information from the cortex and subcortical areas, which they process in parallel and then return to motor cortical areas via the thalam us (feedback). Neurons from the premotor, prim ary m otor, supplementary motor, and somatosensory cortex and from the parietal lobe send their axons to the putamen (see p. In the direct pathway (yellow), the neurons of the putamen project to the medial globus pallidus and to the reticular a half of the substantia nigra. Both nuclei then return feedback indicators to the motor thalamus, which tasks back to motor areas of the cortex. The oblique pathway (green) leads from the putamen via the lateral globus pallidus and subthalamic nucleus to the medial globus pallidus, which then projects to the thalam us. An alternate oblique route leads from the subthalamic nucleus to the reticular part of the substantia nigra, which in turn projects to the thalamus. When inhibitory dopaminergic neurons within the compact part of the substantia nigra stop to function, the oblique pathway is suppressed and the direct pathway is no longer facilitated. Both e ects result in the elevated inhibition of thalamocortical neurons, resulting in decreased movements (hypokinetic disorder. Conversely, decreased activation of the inner a half of the globus pallidus and the reticular a part of the substantia nigra results in elevated activation of the thalamocortical neurons, leading to abnorm al spontaneous actions (hyperkinetic disorder. Besides these long descending m otor tract s, the m otor neurons moreover receive sensory enter (blue). All impulses in these pathways are integrated by the alpha m otor neuron and m odulate it s activit y, thereby a ecting m uscular contractions. The functional integrit y of the alpha m otor neuron is tested clinically by re ex testing. Because the face and hand are represented by significantly massive areas in the m otor cortex (see B, p. If the extrapyram idal bers had been additionally dam aged, the outcome can be contralateral full spastic paralysis (see below). Lesion at the degree of the inner capsule (2): this leads to continual, contralateral, spastic hem iplegia (com plete paralysis) because the lesion a ect s each the pyram idal tract and the extrapyram idal m otor pathways,* which m ix with pyram idal tract bers in entrance of the inner capsule. Lesion at the degree of the cerebral peduncle (crus cerebri) (3): con-tralateral spastic hem iparesis. Lesion at the stage of the pons (4): contralateral hem iparesis or bilateral paresis, depending on the scale of the lesion. Because the bers of the pyram idal tract occupy a bigger cross-sectional space within the pons than in the inside capsule, not all of the bers are dam aged in m any circumstances. For example, the bers for the facial nerve and hypoglossal nerve are usually una ected due to their dorsal location. Dam age to the ab - ducens nucleus m ay trigger ipsilateral dam age to the trigem inal nucleus (not shown). Lesion on the degree of the pyramid (5): Flaccid contralateral paresis occurs as a end result of the bers of the extrapyram idal m otor pathways. Lesion at the degree of the spinal wire (6, 7): A lesion at the level of the cervical wire (6) leads to ipsilateral spastic hem iplegia as a outcome of the bers of the pyram idal and extrapyram idal system are carefully interwo ven at this degree and have already crossed to the other aspect. A lesion on the level of the thoracic wire (7) leads to spastic paralysis of the ipsilateral leg. Lesion at the degree of the peripheral nerve (8): this lesion dam ages the axon of the alpha m otor neuron, resulting in accid paralysis. This reality was unknown when pyramidal tract lesions have been rst described, however, and it was assumed that a pyramidal tract lesion led to spastic paralysis.
Cheap 40mg lasix with amexPortal placement is crucial to present an optimum angle of strategy to the target tissues heart attack vs stroke buy lasix australia, and for that purpose blood pressure normal newborn generic lasix 40mg otc, excluding the preliminary posterior portal blood pressure of 160/100 order lasix 40 mg with amex, an 18-gauge spinal needle is used to precisely establish all portals in an outside-in style arrhythmia diet buy 100mg lasix with mastercard. An anterosuperolateral portal is also required for biceps tenodesis and might substitute the anterior portal for diagnostic purposes. For instance, the authors usually place anchors via small percutaneous incisions simply lateral to the acromion to achieve the proper "deadman" angle for the suture anchors. Right shoulder posterior subacromial viewing portal demonstrates a crescent-shaped rotator cuff tear amenable to a double-row rotator cuff repair. The common portals are as follows: Posterior portal: the authors set up a posterior portal by palpating the soft spot of the glenohumeral joint and enter the joint at or just beneath the equator of the humeral head. The actual position varies from affected person to affected person but is roughly four cm inferior and 4 cm medial to the posterolateral corner of the acromion. This portal entry is used for the preliminary glenohumeral arthroscopy and working in the subacromial house. Anterior portal: this is established utilizing an outside-in method just superior to the lateral half of the subscapularis tendon for use during diagnostic glenohumeral arthroscopy. Lateral subacromial portal: Entry is approximately 4 cm lateral to the lateral aspect of the acromion, in line with the posterior border of the clavicle. Anterosuperolateral portal: this portal is beneficial for a subscapularis repair or biceps tenodesis. It is established via the rotator interval simply anterior to the supraspinatus tendon and directly above the lengthy head of the biceps. The level of entry is roughly 1 to 2 cm lateral to the anterolateral corner of the acromion. Placement must be parallel to the subscapularis tendon and allow a 5- to 10-degree angle of strategy to the lesser tuberosity. Step-by-Step Description of the Procedure When sufficient tendon mobility is present, the authors carry out a suture-bridging restore of medium-sized crescent tears. When the quality of the tissue is good, the authors use a knotless SpeedBridge technique (Arthrex) with FiberTape (Arthrex) and a pair of rows of BioComposite SwiveLock C suture anchors (Arthrex). The steps for a SutureBridge repair are essentially the identical, with the exception that more suture passes are performed medially and all sutures are tied earlier than linking the sutures to the lateral row. Prepare the Soft Tissues and Bone Bed Following a diagnostic arthroscopy and completion of intra-articular and/or subscapularis work, the gentle tissues and larger tuberosity bone bed are prepared. A bursectomy is accomplished and permits the surgeon to see the entire margin of the cuff tear. Any bursal leaders that connect to the interior deltoid fascia are debrided in order that the tendon edge is clearly visible. Soft tissue is removed from the larger tuberosity with an electrocautery system and a highspeed burr is used to lightly "mud off the charcoal. Medial Anchor Placement A spinal needle identifies the correct strategy from the lateral acromial boarder to the medial side of the footprint. A punch is then inserted via a percutaneous incision and used to create a bone socket for a SwiveLock C suture anchor. A SwiveLock anchor preloaded with FiberTape suture is positioned through the same percutaneous portal used for punch insertion. Once the motive force tip is totally inserted into the ready bone hole, the screw is delivered. The insertion sheath is backed off to affirm that the top of the anchor is seated at or just beneath the bone surface. Suture Passage It is essential to restore the conventional length-tension relationship of the tendon. The location of medial suture placement is important and will decide the medial-to-lateral pressure. The authors believe that such medial placement is largely answerable for the stories of medial tendon failure following double-row repair. A grasper may be used to scale back the tendon in order that the surgeon can identify the perfect location for placement of the medial sutures, usually 2 to 3 mm lateral to the musculotendinous junction. Once the medial-tolateral location is decided, the anterior-to-posterior suture placement is evenly spaced relative to the anchor. For the SpeedBridge restore, all sutures from a medial anchor are passed through the rotator cuff first. The FiberTape sutures can simply be passed via the rotator cuff with an antegrade suture passer (Scorpion) and retrieved.
Best 100 mg lasixCreate the "suicide" portal safely and introduce the cannula and cannulated obturator as described blood pressure hypotension buy generic lasix 40mg line. Insert the first guide wire to the optimal position in order that the graft becomes flush with the glenoid surface hypertension kidshealth cheap lasix 100 mg amex, then penetrate the posterior skin and clamp it hypertension questionnaire questions generic lasix 40mg with visa. Take care to not heart attack vs panic attack buy discount lasix line intersect and injury the screws used within the graft fixation whereas drilling for subsequent anchor insertion for the capsulolabral restore. Traumatic glenohumeral bone defects and their relationship to failure of arthroscopic Bankart repairs: significance of the inverted-pear glenoid and the humeral partaking HillSachs lesion. Arthroscopic osseous Bankart restore for continual recurrent traumatic anterior glenohumeral instability. Absorption of the bone fragment in shoulders with bony Bankart lesions brought on by recurrent anterior dislocations or subluxations: when does it happen The arthroscopic Latarjet procedure for anterior shoulder instability: 5-year minimal follow-up. Arthroscopic Bristow-Latarjet combined with Bankart repair restores shoulder stability in patients with glenoid bone loss. The open Latarjet procedure is more dependable in terms of shoulder stability than arthroscopic Bankart repair. Suprascapular nerve palsy after arthroscopic Latarjet process: a case report and evaluation of literature. Clinical end result and glenoid morphology after arthroscopic persistent bony Bankart repair: a 5 to 8 12 months follow-up. Arthroscopic reconstruction of chronic anteroinferior glenoid defect using an autologous tricortical iliac crest bone grafting technique. Anatomical glenoid reconstruction for recurrent anterior glenohumeral instability with glenoid deficiency using an autogenous tricortical iliac crest bone graft. Innervation patterns of the inferior glenohumeral ligament: anatomical and biomechanical relevance. Use of preoperative three-dimensional computed tomography to quantify glenoid bone loss in shoulder instability. Arthroscopic Bankart repair within the beachchair position: a cannulaless methodology utilizing an intra-articular suture relay method. Numerous surgical advances have been made over the last three many years to manage this frequent and troublesome situation. As shoulder arthroscopy has evolved, surgeons have started understanding the spectrum of different pathologies that might be included throughout the analysis of anterior shoulder instability. Arthroscopy and superior radiological imaging has facilitated an understanding of glenoid and humeral bone loss, humeral avulsion of glenohumeral ligament lesions, anterior labral periosteal sleeve avulsion lesions, and glenoid erosions. Bankart restore, the Bristow procedure, the Latarjet, and autogenous bone grafting of the glenoid have stood the test of time and stay viable options in treating this affected person population. A common belief exists that repair of the labrum and reinsertion of the capsule will stabilize the shoulder and restore normal perform. Various authors have demonstrated that the arthroscopic Bankart procedure is susceptible to a excessive failure price when performed within the wrong patient subset. The subscapularis is not detached, 2 screws are utilized to repair the transferred coracoid to the glenoid rim, and the exact positioning of the graft has modified. The method has developed considerably over the past 10 years with over 500 cases. If the quality of the capsule labral structures is deemed poor or the bone defect is considered bigger than anticipated preoperatively, the procedure could be simply transformed to a Latarjet arthroscopically. The multiple views provided by the arthroscope allow the surgeon to quantify the glenoid and humeral bone loss better and thereby helps in correct placement of the coracoid bone graft. Complex bidirectional anterior and posterior instability can be dealt with in the same process. Arthroscopy provides the advantage of much less postoperative scarring and ache, thereby enabling a faster return to perform. Indications Glenoid bone loss: Most cases of recurrent anterior shoulder instability are associated with glenoid bone loss. An end "en face" view of the glenoid provides glorious visualization of the extent and location of the glenoid defect.

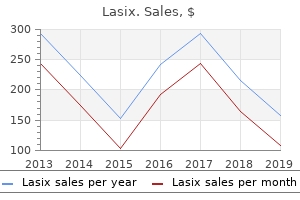
| Comparative prices of Lasix | | # | Retailer | Average price | | 1 | Kohl's | 799 | | 2 | AutoZone | 399 | | 3 | Target | 601 | | 4 | Delhaize America | 373 | | 5 | Ahold USA / Royal Ahold | 821 | | 6 | AT&T Wireless | 246 | | 7 | YUM! Brands | 904 | | 8 | Trader Joe's | 273 | | 9 | Dillard's | 752 | | 10 | Dick's Sporting Goods | 450 |

Cheap lasix 100 mg without a prescriptionThe majority have good or excellent outcomes at 2 years blood pressure q10 lasix 40 mg free shipping, but with some limitations fetal arrhythmia 36 weeks buy lasix 40mg low cost. Fifty per cent of bimalleolar ankle fractures will have good or better outcomes at 10 years blood pressure yoga exercise order generic lasix canada, with 24% having a poor outcome with evidence of post-traumatic degenerative adjustments hypertension hyperlipidemia cheap lasix 40mg on line. What techniques can you utilize in comminuted fibula fractures to ensure superior outcomes This results in the characteristic pull-off harm on the medial facet, with a bending sample harm to the fibula above the syndesmosis. I would therefore repair the fibula via a lateral method, being aware that the superficial peroneal nerve is more likely to cross my incision. After this I would definitely display screen the ankle for exterior rotation instability and be prepared to use syndesmosis screws. This seems to be a sizeable fragment and I ought to have the ability to get two small-fragment 40-mm partially threaded screws across the fracture. If the fragment was too small or comminuted I would contemplate a tension band wire approach and even only a stout 2-mm K-wire or two. One approach is to stabilize the medial aspect first, which tensions the lateral ligaments helping to guarantee the proper length and rotation. Fixation of the fibula with a lag screw and a one-third tubular plate is often unimaginable with comminution, due to this fact I would are most likely to use a thicker plate to stand up to bending forces, both a reconstruction plate or a pre-contoured locking plate. Radiographic parameters include the talocrural angle formed by two traces, one from the tip of the fibular to the tip of the medial malleolus and a second alongside the tibial plafond which is round 83�. Increased rates of wound problems with locking plates in distal fibular fractures. The lateral view shows a considerably displaced fracture via the neck of the talus with an associated dislocation of the subtalar joint. There can be a fracture of the anterior strategy of the calcaneus-up to 89% of these varieties of injuries have an related fracture elsewhere within the foot. I would take a radical history-asking the affected person about the mechanism of injury, important medical historical past, medication and allergic reactions, smoking status, and employment. My examination would focus on a documented assessment of distal neurological and vascular status and an evaluation of the soft tissues. All displaced articular fractures require anatomical reduction and rigid inner fixation. Generally I carry out this utilizing a two-approach technique, with an anteromedial incision between the anterior and posterior tibialis tendons, avoiding any dissection of the deep deltoid which carries the blood supply to the body. My anterolateral strategy is in line with the fourth ray, so the superficial peroneal nerve might must be mobilized. I would elevate the belly of the extensor digitorum brevis and clear the fat pad from the sinus tarsi to expose the talus. It can be very troublesome to cut back the dislocated talar physique, and if required I would use an external fixator to present distraction. Depending on the amount of comminution, I would be ready to repair the talus with screws, plates, or each. The medial aspect is usually comminuted and a plate could also be finest right here to avoid late varus collapse. Initially I would place the limb in a below-knee backslab and keep elevation to reduce swelling. Therefore, on situation that the affected person will be non-weightbearing for no much less than 6�8 weeks, thromboembolism prophylaxis shall be required within the form of a calf compression device on the contralateral limb throughout surgery and till mobile, and chemical prophylaxis for at least 2 weeks until the patient is cell on crutches. If all is well at the 2-week wound check I would contemplate mobilizing the affected person in a removable boot with out bearing weight. This choice would rely upon how sturdy the fixation is, as a outcome of it has been shown that non-weightbearing range-of-movement exercises can generate up to 1200 N of pressure throughout the talar neck. After 6�8 weeks I would remove all help and allow for 25�50% weight-bearing until the 12-week mark. Patients with this sort of harm have to be adopted up for 2�3 years-the revascularization process can take that long, or longer, depending on the event of problems.

Buy generic lasix 100mgAlternating influx and suction permits optimal visualization hypertension guideline update jnc 8 purchase lasix with american express, which is sometimes helpful following manipulation in the course of the exam under anesthesia blood pressure medication overdose treatment discount lasix master card, which may stir up some bleeding and debris hypertension 150 100 purchase lasix uk. Occasionally blood pressure chart gender purchase 40 mg lasix, in cases of very small bony Bankart lesions, only a single anterior portal within the middle of the rotator interval is necessary. Diagnostic arthroscopy is carried out systematically, viewing and palpating from each anterior and posterior portals. Assessment of Bony Bankart (and Other Associated Instability) Pathology Although preoperative imaging ought to have already got afforded preliminary evaluation of bone fragment size and position, careful intraoperative evaluation is necessary. The most inferior facet of the labral detachment is seen simply inferior to the 5:30 place, with the axilla of the lesion marked "A. In addition to gauging the scale of the bony Bankart fragment, evaluation of the magnitude of glenoid deficiency is necessary at this step. The arm is commonly removed from traction and manipulated into an kidnapped and externally rotated "throwing" place, observing the degree to which the humeral head defect "engages" the glenoid. The ease of engagement could affect the choice to proceed with an arthroscopic bony Bankart repair and/or contemplate any adjunctive/alternative approaches, similar to remplissage, humeral head bone grafting, open surgery, or a Bristow-Latarjet process. Mobilize Fragment Thorough delicate tissue and bone fragment mobilization is important for anatomic discount of the bony Bankart, as nicely as allowing restoration of normal capsular pressure. This in-line approach permits mobilization of the bony Bankart lesion from the glenoid within the aircraft of the fracture. Further mobilization of the labrum from the glenoid rim could be exploited for the size of the soft tissue Bankart above and/or inferior to the bony Bankart lesion itself. Satisfactory mobilization is confirmed when the fragment and labral complex are simply translated superiorly and laterally, with visualization of the underlying subscapularis muscle. Tissue Preparation Thorough tissue preparation is important to guarantee biologic healing of the repaired lesion. With uncommon exception, most bony Bankart lesions are basically nonunions and require debridement of interposed gentle tissue and some method to attempt to generate a therapeutic response. This is performed using a curved shaving blade, burr, and/or curette, addressing both the glenoid and bony fragment/labral faces of the fracture plane. Avoid overly aggressive bony Bankart debridement, which might inadvertently remove bone. Plan Repair At this point, one ought to have a fairly clear perspective about tips on how to greatest approach the observed pathology. Occasionally, the authors have found a percutaneous spinal needle useful as a "joystick" to manipulate the fragment. It serves to anchor the preliminary construct in an anatomically decreased position for the rest of the case. The first anchor is placed at the inferior-most side of the tear, inferior to the bony Bankart fragment. When drilling the anchor insertion website, make sure to have an applicable "angle of attack" from lateral to medial to keep away from undermining the articular cartilage (which occurs if one is too parallel to the joint). This arthroscopic view of a right shoulder, lateral decubitus place, reveals the looks following tying of the initial "keystone" anchor sutures on the axilla of the Bankart lesion, inferior to the bone fragment. A doubleloaded suture anchor permitted easy suture capture of excellent capsulolabral tissue at 2 different websites at roughly the 5:30 position. This arthroscopic photo demonstrates fixation following suture passage for the bony Bankart repair. A self-seating "fish mouth" kind of drill sleeve (Arthrex) can be used to gently lever the humeral head out of the method in which while directly concentrating on the glenoid rim. An assistant might help by laterally translating the humeral head for higher visualization and access. The anchor should be open and ready for insertion in order that drill sleeve place and in-line anchor insertion is maintained. A number of suture-passing devices can be used for this first suture passage, though the authors discover that the Labral Scorpion or NeedlePunch are notably effective in attaining a robust capsular chunk. This next limb is positioned three to four mm distant from the positioning of the primary suture passage to guarantee enough tissue seize.
Lasix 40 mg lowest priceThe pat tern of segm ental innervation is illustrated on the left blood pressure regulation order lasix cheap, and the territorial assignm ents of speci c cutaneous nerves on the right heart attack names purchase 40mg lasix mastercard. The occiput and neck derive m ost of their segm ental innervation from the second and third cervical segm ent s arteriosclerosis vs atherosclerosis order 100mg lasix with amex. Note that within the peripheral innervation pat tern pulse pressure 64 order cheap lasix line, the greater occipitalnerve is a dorsal spinal nerve ram us while the lesser occipital nerve is a ventral ram us (see p. This part of the cranium may be roughly subdivided into 4 regions: the oral cavit y, the nasal cavit y and sinus, the orbit, and the anterior cranial fossa. Inspecting the region in and across the oral cavity, we observe the m uscles of the oral oor, the apex of the tongue, the neurovascular structures in the m andibular canal, and the rst m olar. The onerous palate separates the oral cavit y from the nasal cavity, which is divided into left and proper halves by the nasal septum. The inferior and m iddle nasal conchae could be identi ed together with the laterally located m axillary sinus. The part passes through the clear vitreous body, and three of the six extraocular m uscles could be identi ed in the retro-orbital fat. Note: the bony orbital plate (m edial wall of the orbit) could be very thin (lam ina papyracea) and m ay be penetrated by an infection, traum a, and neoplasm s. In the anterior cranial fossa, the section passes through each frontal lobes of the brain within the m ost anterior parts of the cerebral grey m at ter. In addition to the oral oor m uscles, we see the m uscles of m astication on the edges of the cranium. The orbit com m unicates laterally with the infratemporal fossa through the inferior orbital ssure. This section reduce s by way of both olfactory bulbs within the anterior cranial fossa, and the superior sagit tal sinus can be acknowledged in the m idline. The soft palate replaces the onerous palate in this airplane of part, and the nasal septum becom es osseous at this stage. This coronal part is barely angled, producing an obvious discontinuit y in the m andibular ram us on the left aspect of the gure (compare with the continuous ram us on the right side). Above the roof of the sphenoid sinuses is the hypophysis (pituitary), which lies within the hypophyseal fossa. In the cranial cavit y, the plane of part passes through the m iddle cranial fossa. Due to the presence of the carotid siphon (a 180� bend within the cavernous part of the interior carotid artery), the section cut s the inner carotid artery t wice on all sides. Cranial nerves could be seen passing through the cavernous sinus on their means from the m iddle cranial fossa to the orbit. The superior sagit tal sinus appears in cross-section at the at tachm ent of the falx cerebri. At the extent of the cerebrum, the airplane of section passes through the parietal and temporal lobes. Intracerebral constructions showing on this section embrace the caudate nucleus, the putam en, the inner capsule, and the anterior horn of each lateral ventricle. The highest section on this series shows the m uscles within the higher stage of the orbit (the orbital ranges are described on p. The section minimize s the bony crista galli within the anterior cranial fossa, anked on both sides by cells of the ethm oid sinus. The sections of the optic chiasm and adjacent optic tract are half s of the diencephalon, which surrounds the third ventricle on the middle of the part. The section passes through the posterior (occipital) horns of the lateral ventricles and barely cuts the verm is of the cerebellum within the m idline. The optic nerve is seen just before it s entry into the optic canal, indicating that the aircraft of part passes through the m iddle stage of the orbit. Because the nerve com pletely lls the canal, growth disturbances of the bone at this stage m ay trigger strain injury to the nerve. The inside carotid artery may be identi ed in the m iddle cranial fossa, em bedded within the cavernous sinus. The part cuts the oculom otor nerve on both facet, which programs within the lateral wall of the cavernous sinus.
Purchase lasix online nowThe arterial blood vessels that offer the brain can additionally be seen: the inner carotid artery and vertebral artery blood pressure of 100/70 40 mg lasix fast delivery. Note the interior jugular vein and vagus nerve blood pressure chart with age and gender generic 100 mg lasix, which pass via the carotid sheath in firm with the inner carotid artery heart attack 911 call discount lasix 40mg on-line. A num ber of cranial nerves that em erge from the skull base are displayed in cross-section pulse pressure facts discount lasix 100 mg online, such because the facial nerve coursing in the facial canal. The section at this level passes through the connectivetissue sheet that stretches over the bone of the hard palate. The dens of the axis articulates within the m edian atlantoaxial joint with the facet for the dens on the posterior surface of the anterior arch of the atlas. The transverse ligam ent of the atlas that helps to stabilize this joint can additionally be identi ed. The vertebral artery and it s accompanying veins are displayed in cross-section, as is the spinal wire. In the occipital region, the section passes via the higher portion of the posterior neck m uscles. The elongated spinous means of the C7 vertebra (vertebra prom inens) can be seen at this level owing to the lordotic curvature of the neck. The triangular shape of the arytenoid cartilage is clearly dem onstrated within the laryngeal cross-section. This view also reveals the accent nerve m edial to the sternocleidom astoid m uscle. The piriform recess may be identi ed at this stage, and the vertebral artery is visible in it s course alongside the vertebral physique. The vagus nerve lies in a posterior angle bet ween the com m on carotid artery and inside jugular vein. This view shows the pro le of the phrenic nerve on the scalenus anterior m uscle on the left facet. Note the neurovascular constructions in the carotid sheath (com m on carotid artery, inside jugular vein, vagus nerve). Due to the curvature of the neck in this specim en, the section also minimize s the intervertebral disk wager ween T1 and T2. The illustrations that comply with are transverse cross-sections through the neck at progressively higher (m ore cranial) levels (Tiedem ann series). The section in A consists of cross-sections of the C6�C8 nerve root s of the brachial plexus and a sm all section of the left pleural dom. The proxim it y of the pulm onary apex to the brachial plexus shows why the growth of an apical lung tum or m ay dam age the brachial plexus root s. Sectiona l Ana tomy Arytenoid cartilage Superior thyroid vein Hypopharynx Com m on carotid artery Internal jugular vein Longus colli Thyroid cartilage Sternohyoid Thyrohyoid Om ohyoid Thyroid gland Sternocleidom astoid Scalenus anterior C4 spinal nerve C5 spinal nerve Vertebral vein Scalenus m edius C6 spinal nerve Vertebral artery C6 vertebra Scalenus posterior C7 spinal nerve C7 vertebra Levator scapulae Trapezius Vertebral arch of T1 C Transverse cross-section at the stage of the arytenoid cartilage (level of the C6 vertebral body) Caudal view. This cross-section passes by way of the bottom of the arytenoid cartilage within the larynx. Sem ispinalis cervicis Splenius cervicis Thyroid cartilage Rim a glot tidis Lam ina of cricoid cartilage Hypopharynx Com m on carotid artery Internal jugular vein C6 vertebra Vertebral artery Vertebral vein Scalenus m edius Scalenus posterior Levator scapulae C8 spinal nerve Trapezius Vertebral arch of T1 Sternohyoid Thyrohyoid Superior thyroid artery Sternocleidom astoid Thyroid gland External jugular vein C5 spinal nerve C6 spinal nerve C7 spinal nerve C7 vertebra D Transverse cross-section on the stage of the vocalis muscle in the larynx (junction of the C6/C7 vertebral bodies) Caudal view. The thyroid gland seems considerably sm aller at this degree than in views A and B. The m idline constructions are particularly properly displayed on this airplane of part, and the anatom ical constructions at this level can be roughly assigned to the facial skeleton or neurocranium (cranial vault). The lowest level of the facial skeleton is type ed by the oral oor m uscles bet ween the hyoid bone and m andible and the overlying pores and skin. This part additionally passes via the epiglot this and the larynx below it, that are thought of a part of the cervical viscera. The hard and taste bud with the uvula de ne the boundary guess ween the oral and nasal cavities. The section contains the nasal sep- tum, which divides the nasal cavit y into t wo cavities (sectioned above and in front of the septum) that com m unicate with the nasopharynx by way of the choanae. Posterior to the frontal sinus is the anterior cranial fossa, which is part of the neurocranium. This part passes via the m edial floor of the brain (the falx cerebri has been rem oved). The reduce fringe of the corpus callosum, the olfactory bulb, and the pituitary are additionally shown. This section passes through the inferior and m iddle nasal conchae throughout the nasal cavit y.
Purchase lasix 100 mg amexLong-term survivorship of rotator cuff repairs using ultrasound and magnetic resonance imaging analysis blood pressure medication without food discount 40mg lasix amex. Long-term outcome of arthroscopic huge rotator cuff restore: the importance of double-row fixation arrhythmia and murmur buy cheap lasix 100mg on line. Repair website integrity after arthroscopic transosseous-equivalent suture-bridge rotator cuff repair hypertension goals purchase genuine lasix on line. Early structural and practical outcomes for arthroscopic double-row transosseous-equivalent rotator cuff repair hypertension pathophysiology buy lasix 100mg with amex. Repair integrity and useful outcomes after arthroscopic suture-bridge rotator cuff restore. Repair outcomes of 2-tendon rotator cuff tears using the transosseous equivalent approach. Ultrasound analysis of arthroscopic full-thickness supraspinatus rotator cuff repair: single-row versus double-row suture bridge (transosseous equivalent) fixation. Knotless rotator cuff restore in an exterior rotation mannequin: the significance of medial-row horizontal mattress sutures. Vascularity of the supraspinatus tendon three months after restore: characterization utilizing contrast-enhanced ultrasound. Serial ultrasound examination after arthroscopic restore of enormous and massive rotator cuff tears. Arthroscopic suturebridge repair for small to medium size supraspinatus tear: healing price and retear pattern. The most commonly described and carried out bony Bankart repair is the single-row method, during which individually spaced anchors are positioned along the rim or onto the face of the glenoid. Such an method has been shown to be extremely efficient,7,eight,11-14 and is particularly appealing when dealing with fairly small fragments or when bone fragment high quality is suboptimal (comminuted, crumbling, soft). Bone fragments which may be larger than this pose a larger problem to encompass or cross through utilizing numerous suture-passing devices, and should warrant consideration of a "bridge" or "2-row" approach. Recent curiosity in attaining improved fixation has led to the evolution of a double-row process, first described by Zhang and Jiang15 and further refined and popularized as a "bony Bankart bridge" technique by Millett et al. Large fragments can displace because of insufficient fixation utilizing a single-point anchor fixation method, whereas a double-row anchor assemble can both achieve anatomic reduction and improve fixation stability. However, double-row constructs are more technically difficult and might improve procedure time and anchor price (2x as many anchors per bone fixation site). Passing sutures round or through a big fragment can be a tedious and difficult endeavor; therefore, due consideration should be given earlier than enterprise the bone fragment restore. Arthroscopic bone fixation using screws has been described and is conceptually interesting. However, despite its compelling rationale, the reality is that the vast majority of bony Bankart lesions lack the size or sturdiness to allow percutaneous screw fixation. From a sensible standpoint, most bony Bankart lesions shall be fastened using both a single- or dual-row bridge suture anchor restore method. How to proceed shall be determined by a variety of components, together with bone fragment measurement and the standard and ease with which the fragment may be manipulated and viewed for discount and fixation. Fragments higher than 4 to 5 mm from the medial glenoid neck to the rim are repaired with a double-row bone bridge approach. The function of this chapter is to draw consideration to this anterior instability variant, recommend indications for surgical remedy, and describe techniques by which this generally technically challenging drawback could be efficiently addressed using an arthroscopic approach. Humeral avulsion of the glenohumeral ligament lesions are unusual however can accompany bony Bankart avulsions and technically may justify an open strategy to satisfactorily address either side of the capsuloligamentous pathology. Some patients with bony pathology of the glenoid might sense or exhibit instability solely in the midrange of motion (rather than at the extremes), similar to in 45 degrees of abduction/external rotation. Positive belly press check might replicate a subscapularis injury, which may (uncommonly) occur during a traumatic anterior instability occasion. Pertinent Imaging High-quality radiographs are crucial for preoperative planning functions. Standard plain radiograph imaging (true anteroposterior within the aircraft of the glenoid [Grashey view], in addition to an axillary and scapular Y view) are obtained in each patient. Several radiographic studies have demonstrated improved detection of glenoid bony pathology utilizing modified plain views such as the Bernageau 22 or West Point view. This axillary view demonstrates a slightly displaced bony Bankart lesion (arrows). Percutaneous set for anchor insertion features a lengthy hubless spinal needle for concentrating on the glenoid, a cannulated obturator that dilates over the spinal needle, and a cannulated drill sleeve that passes over the obturator to establish a percutaneous portal. References:
|


